News

Prepartions behind the calibration of the active components of the Dose3D-F phantom prior to setting up the phantom and commencing the actual dose measurement. From the left: Bartosz Mindur, Piotr Wiącek, Jakub Hajduga, Tomasz Szumlak, Dagmara Kulig oraz Damian Kabat
Once emitted, a radiation dose cannot be reversed. But what if we were able to see exactly what it does before it reaches the patient’s body? The Dose-3D project was established so that radiation doses could be assessed many times, but on a phantom. As a result, physicians would be sure to adopt the optimal treatment plan. A prototype of the device is ready, but its launch is far ahead. Professor Tomasz Szumlak from the Department of Particle Interactions and Detection Techniques at the Faculty of Physics and Applied Computer Science, the project manager, spoke to us about its genesis, development, and capabilities.
An interview conducted by Katarzyna Dziadowicz, Centre for Communication and Marketing, AGH University
Apparently, the inspiration for the Dose-3D project was the dream of a medical physicist of a tool that would allow the radiation dose to be checked before its administration to the patient.
That is an interesting story. We were finishing a project in which my group participated as software specialists. The project was concerned with the stability of the calibration procedure. We had to verify the repeatability of the radiation doses. Interestingly enough, the group that was formed then also completed the present project, although they were not related. We were in fact a group of people with experience in designing detectors, and during our last meeting, one of the physicians said that such a great device would be a detector measuring the radiation dose across the entire modelled volume at a single moment and providing real-time information about the deposited therapeutic dose. That spark led to a series of discussions with experts from the National Oncology Institute (NIO) and Cracow University of Technology, which flourished in the acquisition of European funds from the Smart Growth Programme as part of the Team-NET project of the Foundation for Polish Science.
The detector developed by you will be used in photon therapy.
That was the idea at first. That group engaged in the work of the National Oncology Institute, so it started with photon therapy, but now we are cooperating with the Institute of Nuclear Physics to try to use our detector with a proton beam. The patients are safe and the verification is technically high quality, but we could use a device such as our phantom to directly measure the radiation beam in the specified volume. In theory, thanks to such a solution, we could access information on how a beam of those protons exactly looks like. It is obviously not that easy because a proton beam is so powerful (in terms of the energy it may deposit), like... a train. When “entering” into the detector, it could potentially cause damage or cause jet quenching. That is an undesirable phenomenon that may occur in radiation detection systems in the case of heavy-ion collisions (such as a proton beam). We talk about it when the detector’s response to the deposited energy is not linear. Meanwhile, linearity of response is a desirable feature of radiation detection systems. Ion quenching is a truly relevant effect, but, from our perspective, a disadvantageous one.
So far, no one has done so. There were some test studies with scintillators, but no one studied the phenomenon using a device with spatial granularity. Traditionally, scintillators are materials capable of emitting photons (of a wide energy spectrum) in response to energy transferred from radiation interacting with them. These materials may be liquid or solid. In our research, we focus on special, printed scintillation plastics with properties such as tissues. Using such a granularity detector along a proton beam would be a pioneering solution, as up to this point more studies have concerned the interaction of a plastic scintillator with photons. Nevertheless, the phantom looks promising also in the case of protons, so we wish to get to this point, although our work is still in the preliminary stages.
What then does photon therapy consists in?
Radiation therapy with the use of photon beams is one of the treatments used in oncology. Unlike proton therapy, it can be used for very extensive cancerous lesions with complex shapes located in various parts of the body. A significant difference between the two is the method for administering the therapeutic dose that effectively destroys cancerous tissues. In the case of protons, ionisation is more or less constant, and when protons lose a sizeable portion of their kinetic energy, they rapidly lose energy (this is known as the Bragg peak). As a result, proton therapy can be used for shallow tumours, to put it simply. The impact of photons is of a different character, because there are no sudden changes in the deposited energy. Photon therapy compares well with proton therapy because with protons we can precisely control the beam. In this case, we may set the energy and intensity of the beam, and the physical processes related to the deposition of energy are very predictable. We may define the maximum penetration depth for a given energy. For protons, we are able to plan where up to 99% of the energy will be deposited. That is precisely why such a beam may be used to attack neoplasms that are close to important organs or near the surface, like in the case of eye cancers, but also cancers near the brain, because the tissue to penetrate is not extensive. A problem arises when the neoplasmic change is extensive and deep, as in the case of soft tissues such as the lungs. This is where the problem begins for proton therapy, because then the ionisation process also affects all healthy tissue “on its way” and is quite intense, as the beam penetrates it to reach such a depth. That is why when we see extensive, deep changes, we turn to photon therapy. In photon therapy, the photon beam is produced by a beam of electrons bombarding a selected element made of a heavy metal (e.g. wolfram). Electrons are rapidly stopped, effectively producing X-ray radiation. Actually, the system is similar to an X-ray lamp, but obviously with a different energy and intensity of the beam. When producing the photon beam, such a machine creates an immediate problem because I cannot control the photon beam like I did with protons. These are uncharged particles, the beam created is wide, and the photons do not have a determined energy but a whole spectrum because the process of stopping electrons is rampant. Using the proton beam, I can scan a selected area, very easily set a magnetic field to just move up and down, and also change the energy. Whereas, in case of the photon bean, I cannot do such things; photons cannot be controlled like that. The trick is to properly condition this photon beam: you have to flatten it, try to align it somehow, additionally, if we start talking about aspects such as the treatment of extensive cancer, such a cancer may come in different shapes, so a very big complication is the field shaping itself. These are very complex systems of the so-called multileaf collimators (MLC), which are arranged in quite a specific shape. We also must take into account that this beam is projected over a certain distance. The beam is not controlled, so it will be divergent, just like when we are casting shadows on a wall: the further we are, the more they change – they become larger and blurrier. So, we need very advanced tools that will model what the projection of this beam will look like, the projection of the collimator opening onto the patient's body. And these are all the complications involved in adapting this beam so that it becomes a therapeutic beam. Also, it is not easy to prepare this beam so that it has a constant intensity. I have a certain therapeutic area, and basically when we produce this photon beam, it is like a spherical wave – it has an irregular shape at its front. Additionally, while heavy charged particles, such as protons, have constant ionisation in the penetration depth, and when the particle stops, virtually all of its energy is deposited in that exact point, in the case of photons we have a continuous and highly variable deposit. This beam deposits energy in a more exponential manner, meaning that we do not have a fragment of a fixed deposit with a maximum deposit somewhere, but rather a constant weakening of this photon beam. And this is another problem, because we cannot attack this change from one angle, from one position. A treatment plan should be developed that will radiate the area from several or even dozens of different angles – from above, below, from the side – so that the lowest possible dose of energy is deposited in healthy tissue and a high dose is deposited only in the diseased area.
Therefore, if a patient comes to a doctor with a diagnosis, a discussion with specialists in the field of medical physics must come first. The area where the therapeutic dose will be deposited must be defined very precisely. There are special computer programmes that perform simulations and then work out the best way to deliver that dose – they calculate the best directions from which to radiate the area, avoiding vital organs, so that we have the maximum deposit in the area where the diseased tissue is located. That is what it looks like in a nutshell.
What we are striving for in our project is to have a device that is very well prepared to accurately measure spatial dose distribution and that will allow us to show that our simulations are consistent with reality. Normally, such verification is not possible because it is impossible to insert anything into a patient undergoing therapy that would allow direct measurement of the deposited radiation doses. Until now, this has been based on calibration of the device, analysis of data from phantoms and simulations, but the phantoms used so far have had limited capabilities. In the currently used phantoms, we have a probe that changes position several dozen times, for example, to measure a certain volume, or there are phantoms made of a material that changes its properties because of radiation. Then the phantom must be taken for the readout, which is overly complicated and usually unstable because it is susceptible to change as a result of external factors such as temperature or time.
Our idea is to create a device with appropriate segmentation that will enable spatial measurement in real time. We will place our phantom on the therapeutic beam and will be able to model the location of the diseased area inside. We could even do this for an individual patient – read the location of the affected area from a CT scan, see what it looks like, and model it in our phantom, and then use the phantom to check the entire treatment plan and perhaps even make specific adjustments.
So, do we physically have a phantom at which we point the photon beam and use software to mark the lesions?
Precisely. The phantom is divided into small voxels, and using software, I mark which voxels are inside the lesion and which are outside. In classic phantoms, this is not done – there is usually one exposure, calibration is performed, and the devices are verified. With a phantom such as the one we have developed, we can prepare a treatment plan customised to the patient, carry it out on the phantom, and accurately measure the radiation dose at the place that represents a lesion in the phantom, as well as its spatial distribution.
The Dose3D-Future team. From the left: Bartosz Mindur, Damian Kabat, Tomasz Szumlak, Piotr Wiącek, Stefan Koperny, Tomasz Fiutowski, Dagmara Kulig, Maciej Kopeć and Andrzej Korba


The Dose3D-F phantom ready for measurements inside a certified I'mRT phantom. In this measurement, a complete treatment plan was carried out. The Dose3D-F phantom represents the critical organ and the irradiated organ.
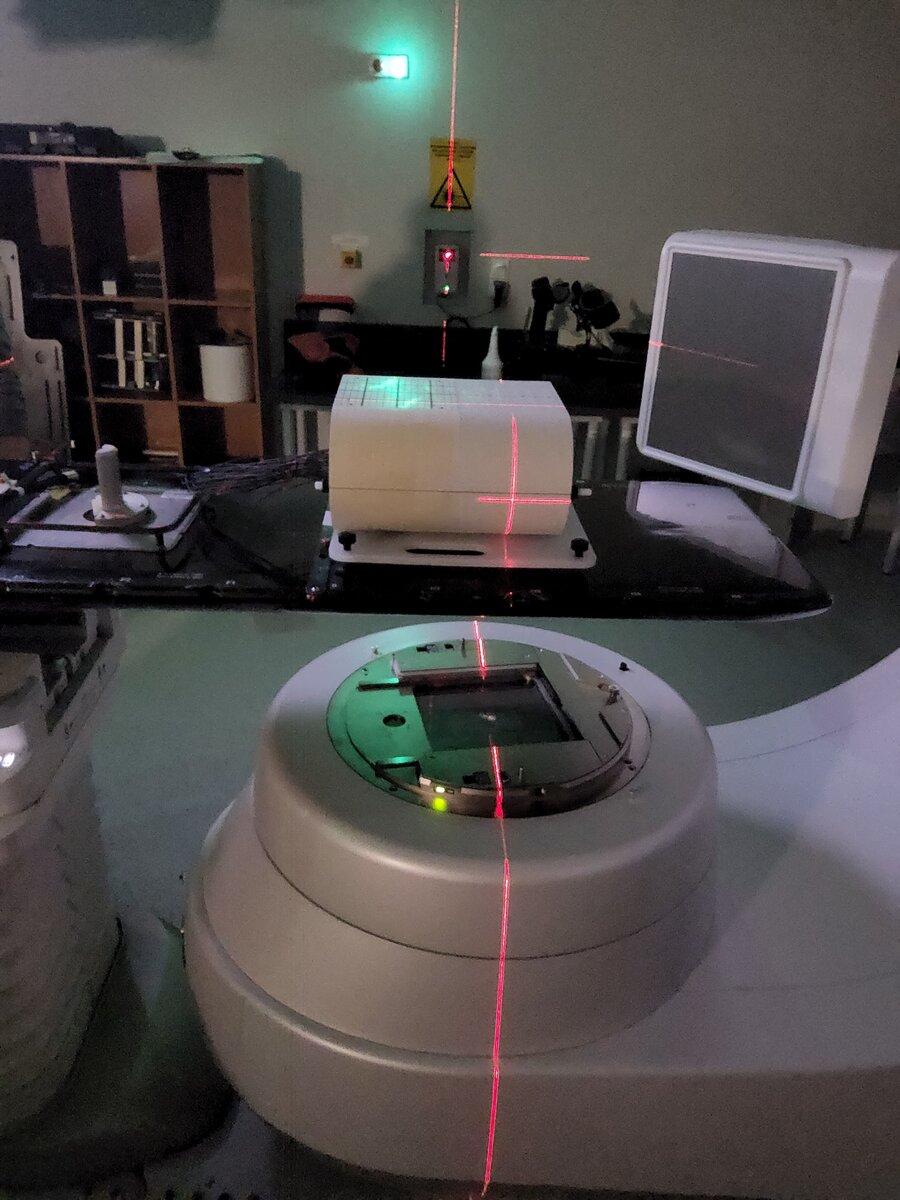
The Dose3D-F phantom was prepared for measurements inside a certified I'mRT phantom. Positioning of the device using a medical laser accelerator system.

Measurement of the spatial distribution of a therapeutic dose using the Dose3D-F phantom in an aquatic environment. This measurement allows for the so-called electron equilibrium conditions to be achieved and represents a realistic patient radiation process (in the foreground, there is an electronic data acquisition system created by researchers from AGH University).

Preparations for the second exposure of the active elements of the Dose3D-F phantom prior to the configuration of the phantom and the actual dose measurements.
 Twelve universities and Krakow Municipality join forces for accessibility
Twelve universities and Krakow Municipality join forces for accessibility  AGH Solar Plane develops fast and agile Rico plane
AGH Solar Plane develops fast and agile Rico plane  AGH University and the National Museum in Krakow to cooperate in the field of AI
AGH University and the National Museum in Krakow to cooperate in the field of AI  Leading AI researchers to meet at AGH University
Leading AI researchers to meet at AGH University  AGH University at the 3rd Poland–Uzbekistan Rectors’ Forum
AGH University at the 3rd Poland–Uzbekistan Rectors’ Forum  AGH University at European Economic Congress
AGH University at European Economic Congress  Become an analog astronaut: call for applications for NAWA UNIVERSEH OPEN
Become an analog astronaut: call for applications for NAWA UNIVERSEH OPEN 